第八章 腎臟損傷與修復
第一節 腎臟損傷的定義及分類
腎臟損傷是指由內源性或外源性因素所引發的腎臟結構和/或腎臟功能受損。其發病機制涉及免疫反應及非免疫反應。
腎臟損傷種類多樣,根據病程、病因及嚴重程度進行分類。按病程長短可分為:急性腎損傷,慢性腎臟病;按病因可分為原發性腎臟疾病,繼發性腎臟疾病;其中繼發性腎臟疾病因致病因素不同,可細分為以下種類:外傷所致腎損傷、藥物性腎損害、梗阻性腎損害、環境或職業因素所引起的腎損害、感染性疾病所致腎損害、自身免疫性疾病及結締組織疾病腎損害、代謝性疾病腎損害、副蛋白血癥病腎損害、腫瘤相關腎損害;按損傷主要部位可分為腎小球疾病、腎小管疾病、腎間質疾病及腎血管疾病;按腎功能損傷嚴重程度,其中慢性腎臟病按照腎小球濾過率下降程度可分為5期:正常、輕度下降、中度下降重度下降、腎衰竭,其中的中度下降期又細分為輕中度下降期和中重度下降期[1];急性腎損傷按照2012KDIGO發布的最新標準可分為1期、2期、3期[2]。
第二節 腎臟損傷的作用機制
各種原因引起的腎臟損傷與腎臟病發生,發展有著十分密切的關系。目前研究證實腎臟損傷的作用機制復雜,目前可分為兩大類:免疫[3-5]及非免疫[6-9]機制。臨床上常見的腎小球疾病多為免疫介導,主要包括:體液免疫及細胞免疫。體液免疫主要指B淋巴細胞介導的抗原抗體反應,而細胞免疫主要指T淋巴細胞所介導的免疫調節作用,如單核/巨噬細胞活化等所引起的細胞因子,活性氧代謝產物,蛋白酶等釋放所引起的腎臟損害。目前證據表明體液免疫及細胞免疫共同在腎小球疾病中發揮了重要作用[10-13],圖2-8-2-1描述了免疫性腎損傷的發生途徑。
由圖2-8-2-1可知,以下2種方式造成免疫性腎臟損傷:①體液介導免疫腎臟損傷:其發病機制表現為免疫球蛋白或免疫復合物在腎臟的沉積,導致補體激活,引起中性粒細胞及血小板聚集及腎小球內皮細胞脫落;在免疫損傷過程中,活化的巨噬細胞/系膜細胞/中性粒細胞/血小板及受損的內皮細胞大量釋放氧化物、蛋白酶,進一步造成腎小球毛細血管及腎小管上皮細胞的損害,導致蛋白尿及新月體的形成。②細胞介導免疫腎臟損傷:當腎臟損傷時,致敏細胞(主要是T淋巴細胞)可進一步激活巨噬細胞/系膜細胞,繼而引起大量炎癥和生長因子、氧化物、蛋白酶的釋放,造成腎小球毛細血管和腎小管上皮細胞的損害,導致蛋白尿及新月體的形成。
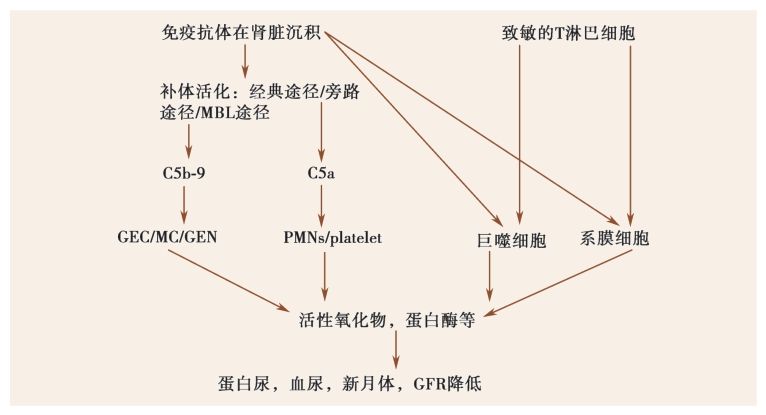
圖2-8-2-1 免疫性腎損傷發病機制
多數免疫性腎臟疾病的病因不清,既有外來因素所引發,也有自身免疫因素及遺傳因素的參與。目前常見的外來因素所引發的免疫性腎臟疾病,多見于感染后的急性腎小球腎炎,乙型肝炎病毒相關性腎炎,丙型肝炎病毒相關性腎炎,藥物性間質性腎損害等;經典的自身免疫性疾病如抗腎小球基底膜病、狼瘡性腎炎、ANCA相關性腎炎。不論免疫性腎臟疾病始動病因如何,最終造成的腎臟損害還同時受到患者遺傳背景因素的影響,遺傳背景與患者的易感性,疾病的嚴重程度,治療反應及預后密切相關。總而言之,上述三種因素是導致免疫性腎臟疾病發生的重要病因。
第三節 腎臟修復的定義、分型、作用及機制
一、腎臟修復的定義及形式
何謂腎臟修復?簡單而言,就是腎臟結構受到損害后自我恢復的一種過程。腎臟組織與腦及心臟等不同,腎組織急性受損后可以依靠存活細胞的自我增殖完全修復,恢復腎功能[14]。但實際上,臨床上急性腎損傷完全恢復的比例很少,相當比例的患者會慢慢逐步進展到慢性腎臟病[15],這與預先存在的慢性腎臟損害[16]及腎損傷的嚴重程度,持續時間及恢復情況有關。腎臟損傷后,有以下幾種修復形式:一是具有細胞增殖導致功能組織的恢復;二是細胞外基質的增生導致瘢痕組織形成;三是通過再生修復的過程重啟原始組織結構的恢復[17]。既往的研究對于腎臟修復主要是集中在細胞外基質增生所導致的腎臟間質纖維化這一領域,而近些年隨著對急性腎損傷研究領域的展開,人們已經把研究熱點開始轉向細胞修復和組織重構方面[18]。在本章節中,我們主要集中在急性腎損傷受損腎小管上皮細胞再生增殖修復領域上。
二、腎臟修復在腎臟損傷中的作用
隨著近年來急性腎損傷的定義,診斷標準全球化,急性腎損傷的發病率及重要性越來越受到大家重視,目前急性腎損傷已成為慢性腎臟病的重要危險因素[19,20]。研究表明腎臟體積及單位的喪失,血管功能不全,細胞周期的異常及不適當的腎臟修復機制都是導致腎臟病進展的重要因素[20]。目前臨床對于急性腎損傷的防治仍缺乏特殊有效的方法,急性腎損傷已成為重癥患者死亡的重要原因[21,22];社區獲得性急性腎損傷的發生率也逐步顯著增加,已成為當今世界一項重要的公共健康問題[23]。
由于急性腎損傷是一種早期可以自我修復的可逆性疾病,因此近年來如何促進急性腎損傷細胞再生修復已成為全球關注的研究熱點。研究表明,動物及人類組織都具有細胞再生修復的能力。事實上,急性腎小管損傷后,大部分健存的腎單位組織已經開始啟動細胞再生修復這一過程,所有的動物種類自原始胚胎腎組織開始都長期保留有這一能力。急性腎損傷后的再生修復主要是指細胞再生修復這一過程[17];最重要的受損腎單位組織結構的完全修復目前只在低等動物中觀察到[24],在成熟的哺乳動物中未觀察到這一現象[25]。
在腎臟的修復過程中,細胞增殖再生修復所引起的功能組織的恢復具有特別重要的意義,有利于加速腎臟損傷的恢復進程,促進腎功能好轉,這一點已被很多研究證實[26]。目前研究表明受損腎臟小管,小球及間質均存在修復,并且受到多種因素的調控影響。
受損腎臟細胞再生修復受到多種因素的影響,如細胞因子、腎臟來源的祖/干細胞[27]和信號通路等[28-32]。腎小管上皮細胞是腎臟結構中最重要的一種細胞,腎小管上皮細胞的損傷程度與腎臟功能喪失密切相關[33]。腎臟急性受損后,損傷區域周圍的腎小管上皮細胞立即啟動修復機制,喪失細胞刷狀緣,去分化成間充質表型。去分化后的小管細胞遷移到細胞壞死/凋亡或裸露的小管基底膜等區域,然后增殖,再分化成上皮樣細胞,完成修復[26]。圖2-8-3-1闡述了缺血再灌注急性腎損傷腎小管上皮細胞正常修復的過程。
腎臟細胞再生修復的程度及形式對于腎損傷的恢復及預后具有非常重要的作用:適應性好的修復能夠恢復腎小管上皮細胞的完整性,腎功能得到完全恢復;適應性差的修復,如不完全的腎小管上皮修復,持續的小管-間質炎癥,成纖維細胞的增生及細胞外基質的沉積等,最終形成慢性腎臟病,甚至可進展到終末期腎臟病(圖2-8-3-2)。
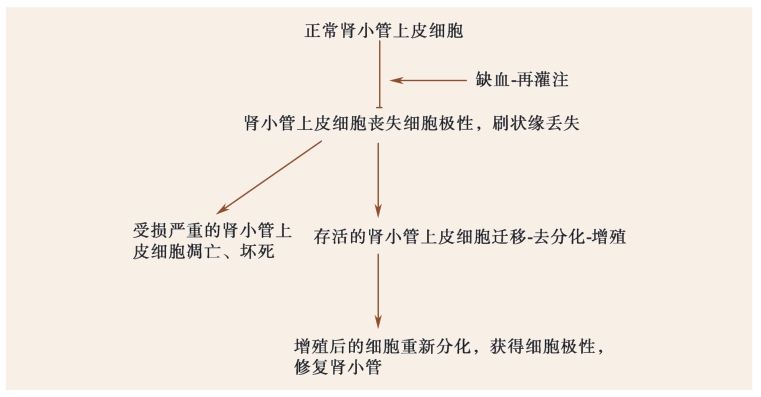
圖2-8-3-1 缺血再灌注急性腎損傷腎小管上皮細胞正常修復
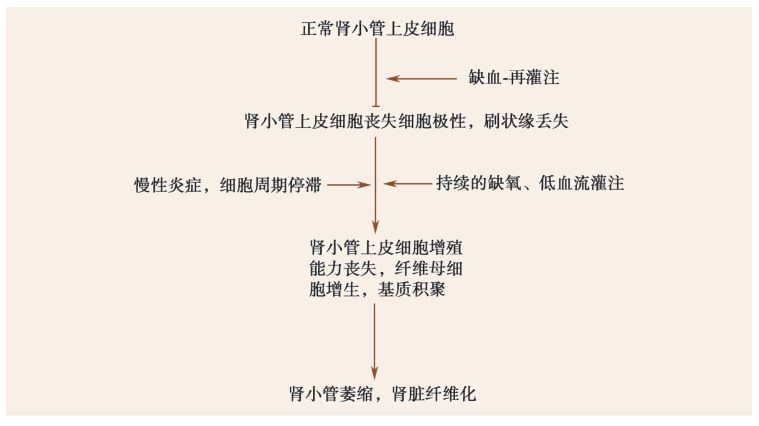
圖2-8-3-2 缺血再灌注急性腎損傷腎小管上皮細胞異常修復
三、腎臟修復的機制
大量研究表明腎臟組織具有一定的自我修復的能力,促進腎臟組織修復能夠顯著改善腎臟病的預后,加速急性腎損傷恢復,延緩慢性腎臟病進程。因此,積極尋求受損腎臟再生修復的機制已成為當前腎臟病領域的研究重點。
近年來關于腎臟損傷后增殖修復腎小管上皮細胞主要起源于何種細胞一直備受爭議,成為目前急性腎損傷再生修復的研究熱點。目前研究表明,腎臟局部存活的上皮細胞[34,35],骨髓間充質干細胞[36,37],和腎臟祖細胞[35,38-40]都可能增生分化成腎小管上皮細胞。有研究指出骨髓間充質干細胞并不直接分化形成腎小管上皮細胞,而是通過對內環境的調整,以旁分泌方式促進腎小管上皮細胞的再生增殖[41,42]。也有研究發現,腎小管上皮細胞的修復來源于腎臟局部稀少,但具有分化能力的祖細胞[43]。所以,急性腎損傷的小管再生修復可能主要是通過局部存活的腎小管上皮細胞[44]去分化-增殖-再分化的過程實現的。
由于腎臟修復是一個復雜的病理生理過程,在整個修復進程中除了再生細胞的來源,參與腎臟細胞修復的內環境因素極其重要。細胞因子,炎癥/免疫細胞,信號通路等交織而成復雜信號網絡在腎臟損傷修復進程中扮演了十分重要的作用。研究表明,腎臟損傷后細胞因子在修復過程了發揮了重要作用[45,46]:其中包括各種促腎生長細胞因子[47]、如肝細胞生長因子[48]、表皮生長因子[49]、胰島素生長因子[50]、肝素結合表皮生長樣因子[51]、血小板衍生長因子[52]、干細胞因子[53]、促紅素[54]、骨形態發生蛋白-7[55]和血管生成因子[56]。也有研究發現轉錄調節因子通過調控參與腎臟修復的因子表達也主動參與了腎臟修復,如Pax-2[57]和Hnf-1beta[58]。不少急性炎癥因子,如C-反應蛋白(CRP),在急性腎損傷患者血清中高度表達,與腎臟不良預后密切相關[59-61]。為了揭示CRP在急性腎損傷中的作用,我們應用人CRP轉基因小鼠,建立了腎臟急性缺血再灌注模型。結果顯示,CRP轉基因小鼠較野生型小鼠腎臟功能及結構損害顯著,予以阻斷CRP后可改善這一情況,促進受損小管上皮細胞增殖[62]。這一結果在體外培養HK-2細胞也得到證實。
眾所周知,腎臟病與免疫炎癥密切相關,腎臟損傷后,各種炎癥/免疫細胞迅速激活并聚集到受損區域:如中性粒細胞[63]、單核/巨噬細胞[64,65]、樹突狀細胞[66]、T淋巴細胞[67,68]等共同參與了急性腎損傷-修復過程。值得注意的是,巨噬細胞[69,70]及T淋巴細胞[67,68,71]因表型不同,在腎臟損傷不同階段發揮了不同作用,這一現象在其他器官損傷中也有同樣發生[72],但具體機制尚不十分明確,值得進一步探討。最近研究發現,調節性T細胞(Treg)在急性腎損傷早期可通過抑制CD4+T淋巴細胞釋放炎癥細胞因子,促進腎臟修復[73];Aghdami等發現在運用骨髓間充質干細胞治療恒河猴急性缺血-再灌注模型時,治療組較對照組腎小管出現大量的Foxp3+的Treg細胞,與腎臟預后密切相關[74]。目前關于Treg細胞在腎臟損傷修復中的作用報道尚不多,待于進一步的研究及觀察。這也讓我們重新審視。在腎損傷-修復進程中除了如前所述的促腎臟細胞增殖修復因子外,同時還有一些負反饋調節因子抑制腎臟修復:如細胞因子信號3的抑制劑[75],反饋調節因子Activin A[76,77]等可抑制腎臟修復,加劇腎臟損害。這些研究結果為將來臨床治療腎損傷提供可能的科學依據。最后,需要提出的是,在整個腎臟損傷-修復進程中,信號通路發揮了不同的重要調控作用。如Wnt、JAK2/STAT[57]、Bcl-2[78]等信號通路參與了腎臟增殖修復的過程。同時,Wnt信號通路的激活也參與慢性腎臟病的修復進程。如過度激活,與腎臟纖維化密切相關[79]。所以,阻斷Wnt信號后可以減輕腎臟纖維化程度[80],改善預后。相反,如敲除巨噬細胞的Wnt7b表達,則顯著抑制了急性缺血-再灌注腎臟小管上皮細胞增殖再生,延緩了腎臟修復[81]。
第四節 減少腎臟損傷、促進腎臟修復的治療手段
近期研究已證實,急性腎損傷是慢性腎臟病的重要原因之一,早期預防及干預急性腎損傷是降低慢性腎臟病發病率、延緩終末期腎病進程及促進腎臟修復的最積極有效的方法。但是,目前臨床對于防治腎臟損傷的手段十分有限,效果也不理想。臨床常見的治療手段還是基于對病因及危險因素的控制:如控制血壓、血糖、水電解質紊亂糾正、腎毒性藥物的慎用、低血容量的糾正、造影劑使用前的水化處理等。
近10年來,由于干細胞在腎臟修復過程中的作用越來越受到重視,越來越多研究者把干細胞治療急性腎損傷放在了極其重要的位置[27,82,83],而且在基礎研究中也得到很好的證實[43,84]。研究發現骨髓間充質干細胞[85,86]、造血干細胞[37]、羊水干細胞[87,88]、腎臟來源的祖/干細胞[89,90]、存活的腎小管上皮細胞[91,92]、內皮祖細胞[93]等均可促進腎臟細胞增殖再生修復,減輕腎臟損傷,改善腎功能。盡管很多基礎研究證實干細胞的運用對于腎臟損傷修復具有很好的效果,但同時也有研究發現,如果補充注入的干細胞長期分化不佳,可以引起腎臟纖維化[94]。除此之外,干細胞療效的程度還受到很多因素的影響,如干細胞干預的時間、干細胞移植的數量、干細胞到達受損區域的能力等。正是由于這些原因的存在使得目前干細胞治療手段在臨床干預治療急性腎損傷還處于探索階段,因此,預計干細胞臨床干預治療腎臟病還有相當長的一段路要走。
需要指出的是,雖然目前很多研究表明骨髓間充質干細胞對腎臟損傷修復有作用,但也有研究者提出不同觀點:促進腎臟損傷修復的并不是間充質干細胞本身,骨髓間充質干細胞不能直接分化為腎臟上皮細胞,而是歸咎于干細胞產生分泌的細胞因子[46,47,95]及干細胞所分泌exosome(膜性小囊泡)[96]等對微環境的影響,刺激促進存活的腎小管上皮細胞去分化或腎臟固有的祖細胞增殖,使受損小管上皮細胞得以修復[97]。因此研究者們又把目光聚焦在干細胞及微環境相互之間的作用對于腎臟損傷修復的影響。有學者發現預先用IGF-1因子預處理的干細胞能促進干細胞的遷移,提高其聚集到受損區域的能力,促進腎臟修復[98]。經CXCR4基因修飾后的骨髓間充質干細胞可通過激活下游的P13K/AKT和MAPK信號通路促進骨髓間充質干細胞遷移到腎損傷區域,加速腎功能的恢復[99]。另外,體內外研究發現,補充EPO可促進干細胞的遷移能力,促進急性腎損傷功能恢復[100]。目前對于干細胞在腎臟損傷修復中的運用還存在很多疑問,如該選取何種干細胞用于干預治療?干預的時間應多長?干預的劑量應多少?內環境的調控因素有哪些?目前尚無統一認識[101,102]。繼續探索干細胞在腎臟損傷修復的作用及相關調節機制仍將是腎臟病研究者們在今后所持續關注重點,這與全球的腎臟病預后密切相關,具有十分重要的意義。
(湯 穎 藍輝耀)
參考文獻
1.ADEERA LEVIN, PAUL E. STEVENS. Retraction: Summary of KDIGO guideline: behind the scenes, need for guidance, and a framework for moving forward. Kidney international, 2013, 85(1): 49-61.
2.KELLUM J A, LAMEIRE N, GROUP KAGW. Diagnosis, evaluation, and management of acute kidney injury:a KDIGO summary(Part 1). Critical Care, 2013, 17(1): 204.
3.KRONBICHLER A, MAYER G. Renal involvement in autoimmune connective tissue diseases. Bmc Medicine,2013, 11(1): 95.
4.COUSER WG. Basic and translational concepts of immune-mediated glomerular diseases. Journal of the American Society of Nephrology Jasn, 2012, 23(3): 381.
5.PONTICELLI C, SALVADORI M, COPPO R. The kidney, a victim and culprit of autoimmune and alloimmune responses. Nephron Clinical Practice, 2011, 119(3): 200-204.
6.ZATZ R, FUJIHARA CK. Mechanisms of progressive renal disease: role of angiotensin II, cyclooxygenase products and nitric oxide. Journal of Hypertension Supplement Official Journal of the International Society of Hypertension, 2002, 20(3): S37-44.
7.ABT AB, COHEN AH. Newer glomerular diseases. Semin Nephrol, 1996, 16(6): 501-510.
8.SUI W, LI H, OU M, et al. Altered long non-coding RNA expression profile in patients with IgA-negative,mesangial proliferative glomerulonephritis. International Journal of Molecular Medicine, 2012, 30(1): 173.
9.BRAUN N, GR?NE HJ, SCHENA FP. Immunological and non-immunological mechanisms of proteinuria.The Italian journal of urology and nephrology, 2009, 61(4): 385.
10.PANI A. Standard immunosuppressive therapy of immune-mediated glomerular diseases. Autoimmunity Reviews, 2013, 12(8): 848-853.
11.GOULD DB, WILLIAMS JW. Acute interstitial nephritis. Kidney International, 2010, 77(11): 956-961.
12.HOLDSWORTH SR, TIPPING PG. Leukocytes in glomerular injury. Seminars in Immunopathology, 2007,29(4): 355-374.
13.COUSER W. Pathogenesis of glomerular damage in glomerulonephritis. Nephrology, dialysis, transplantation:official publication of the European Dialysis and Transplant Association-European Renal Association, 1998, 13 Suppl 1(Suppl 1): 10.
14.JOSEPH V. BONVENTRE, LI YANG. Cellular pathophysiology of ischemic acute kidney injury. The Journal of clinical investigation, 2011, 121(11): 4210.
15.COCA SG, YUSUF B, SHLIPAK MG, et al. Long-term risk of mortality and other adverse outcomes after acute kidney injury: A systematic review and meta-analysis. American Journal of Kidney Diseases the Official Journal of the National Kidney Foundation, 2009, 53(6): 961-973.
16.HSU C, CHERTOW GM, MCCULLOCH CE, et al. Nonrecovery of Kidney Function and Death after Acute on Chronic Renal Failure. Clinical Journal of the American Society of Nephrology, 2009, 4(5): 891-898.
17.ROMAGNANI P, LASAGNI L, REMUZZI G. Renal progenitors: an evolutionary conserved strategy for kidney regeneration. Nature Reviews Nephrology, 2013, 9(3): 137.
18.RICARDO SD, DEANE JA. Adult stem cells in renal injury and repair. Nephrology(Carlton, Vic.), 2005, 10(3):276-282.
19.GOLDSTEIN SL, JABER BL, FAUBEL S, et al. AKI transition of care: a potential opportunity to detect and prevent CKD. Clinical Journal of the American Society of Nephrology Cjasn, 2013, 8(3): 476.
20.CHAWLA LS, KIMMEL PL. Acute kidney injury and chronic kidney disease: an integrated clinical syndrome.Kidney International, 2012, 82(5): 516.
21.WANG X, JIANG L, WEN Y, et al. Risk Factors for Mortality in Patients with Septic Acute Kidney Injury in Intensive Care Units in Beijing, China: A Multicenter Prospective Observational Study. Biomed Research International, 2014, 2014(6): 172620.
22.DHANALAKSHMI P. Epidemiology, outcomes and validation of RIFLE and AKIN criteria in acute kidney injury (AKI) in critically ill patients: Indian perspective. Renal Failure, 2014, 36(6): 831.
23.DE LFV, STUCKER F, SAUDAN P. Epidemiology of community-acquired acute kidney injury. Revue Médicale Suisse, 2014, 10(419): 470-473.
24.REIMSCHUESSEL R. A fish model of renal regeneration and development. ILAR J, 2001, 42(4): 285-291.
25.DAVIDSON AJ. Uncharted waters: nephrogenesis and renal regeneration in fish and mammals. Pediatric Nephrology, 2011, 26(9): 1435.
26.BONVENTRE JV. Dedifferentiation and proliferation of surviving epithelial cells in acute renal failure. Journal of the American Society of Nephrology Jasn, 2003, 14 Suppl 1(90001): S55.
27.MAESHIMA A, NAKASATOMI M, NOJIMA Y. Regenerative medicine for the kidney: renotropic factors,renal stem/progenitor cells, and stem cell therapy. Biomed Research International, 2014, 2014(3): 595493.
28.KULKARNI OP, HARTTER I, MULAY SR, et al. Toll-like receptor 4-induced IL-22 accelerates kidney regeneration. Journal of the American Society of Nephrology Jasn, 2014, 25(5): 978-989.
29.ZHANG MZ, YAO B, YANG SL, et al. CSF-1 signaling mediates recovery from acute kidney injury. The Journal of clinical investigation, 2012, 122(12): 4519.
30.JANG HS, HAN SJ, KIM JI, et al. Activation of ERK accelerates repair of renal tubular epithelial cells,whereas it inhibits progression of fibrosis following ischemia/reperfusion injury. Biochimica Et Biophysica Acta, 2013, 1832(12): 1998-2008.
31.KAWAKAMI T, REN S, DUFFIELD JS. Wnt signalling in kidney diseases: dual roles in renal injury and repair. Journal of Pathology, 2013, 229(2): 221.
32.KWON DS, KWON CH, KIM JH, et al. Signal transduction of MEK/ERK and PI3K/Akt activation by hypoxia/reoxygenation in renal epithelial cells. European Journal of Cell Biology, 2006, 85(11): 1189-1199.
33.VAN KC, DAHA MR, VAN ES LA. Tubular epithelial cells: A critical cell type in the regulation of renal in flammatory processes. Experimental Nephrology, 1999, 7: 429.
34.HUMPHREYS BD, VALERIUS MT, KOBAYASHI A, et al. Intrinsic Epithelial Cells Repair the Kidney after Injury. Cell Stem Cell, 2008, 2(3): 284.
35.MAESHIMA A. Label-retaining cells in the kidney: origin of regenerating cells after renal ischemia. Clinical &Experimental Nephrology, 2007, 11(4): 269-274.
36.KALE S, KARIHALOO A, CLARK PR, et al. Bone marrow stem cells contribute to repair of the ischemically injured renal tubule. Journal of Clinical Investigation, 2003, 112(1): 42-49.
37.LIN F, CORDES K, LI L, et al. Hematopoietic stem cells contribute to the regeneration of renal tubules after renal ischemia-reperfusion injury in mice. Journal of the American Society of Nephrology Jasn, 2003, 14(5):1188.
38.LINDGREN D, BOSTR??M AK, NILSSON K, et al. Isolation and characterization of progenitor-like cells from human renal proximal tubules. American Journal of Pathology, 2011, 178(2): 828-837.
39.ANGELOTTI ML, RONCONI E, BALLERINI L, et al. Characterization of renal progenitors committed toward tubular lineage and their regenerative potential in renal tubular injury. Stem Cells, 2012, 30(8): 1714-1725.
40.MAESHIMA A, YAMASHITA S, NOJIMA Y. Identification of renal progenitor-like tubular cells that participate in the regeneration processes of the kidney. Journal of the American Society of Nephrology, 2003,14(14): 3138-3146.
41.ZHAO JJ, LIU JL, LIU L, et al. Protection of mesenchymal stem cells on acute kidney injury. Molecular Medicine Reports, 2014, 9(1): 91-96.
42.BRUNO S GRANGE, CDEREGIBUS MC, CALOGERO RA, et al. Mesenchymal stem cell-derived microvesicles protect against acute tubular injury. Journal of the American Society of Nephrology : JASN,2009, 20(5): 1053.
43.HARARISTEINBERG O, METSUYANIM S, OMER D, et al. Identification of human nephron progenitors capable of generation of kidney structures and functional repair of chronic renal disease. Embo Molecular Medicine, 2013, 5(10): 1556.
44.YOKOO T. Kidney regeneration with stem cells: an overview. Nephron Experimental Nephrology, 2014,126(2): 54.
45.WISE AF, WILLIAMS TM, KIEWIET MB, et al. Human mesenchymal stem cells alter macrophage phenotype and promote regeneration via homing to the kidney following ischemia-reperfusion injury. American Journal of Physiology Renal Physiology, 2014, 306(10): F1222.
46.FLAQUER M, ROMAGNANI P, CRUZADO JM. Growth factors and renal regeneration. Nefrología, 2010,30(4): 385-393.
47.NIGAM S, LIEBERTHAL W. Acute renal failure. III. The role of growth factors in the process of renal regeneration and repair. American Journal of Physiology Renal Physiology, 2000, 279(1): F3.
48.MATSUMOTO K, MIZUNO S, NAKAMURA T. Hepatocyte growth factor in renal regeneration, renal disease and potential therapeutics. Current Opinion in Nephrology & Hypertension, 2000, 9(4): 395.
49.HUMES HD, CIESLINSKI DA, COIMBRA TM, et al. Epidermal growth factor enhances renal tubule cell regeneration and repair and accelerates the recovery of renal function in postischemic acute renal failure.Journal of Clinical Investigation, 1989, 84(6): 1757-1761.
50.DING H, KOPPLE JD, COHEN A, et al. Recombinant human insulin-like growth factor-I accelerates recovery and reduces catabolism in rats with ischemic acute renal failure. Journal of Clinical Investigation, 1993, 91(5):2281.
51.M SAKAI, M ZHANG, T HOMMA, et al. Production of heparin binding epidermal growth factor-like growth factor in the early phase of regeneration after acute renal injury. Isolation and localization of bioactive molecules. The Journal of clinical investigation, 1997, 99(9): 2128.
52.NAKAGAWA T, SASAHARA M, HANEDA M, et al. Role of PDGF B-Chain and PDGF Receptors in Rat Tubular Regeneration after Acute Injury. American Journal of Pathology, 1999, 155(5): 1689.
53.STOKMAN G, STROO I, CLAESSEN N, et al. Stem Cell Factor Expression after Renal Ischemia Promotes Tubular Epithelial Survival. Plos One, 2010, 5(12): e14386.
54.LIU N, HAN G, CHENG J, et al. Erythropoietin promotes the repair effect of acute kidney injury by bonemarrow mesenchymal stem cells transplantation. Experimental Biology & Medicine, 2013, 238(6): 678.
55.MICHAEL ZEISBERG, JUNICHI HANAI, HIKARU SUGIMOTO, et al. BMP-7 counteracts TGF-|[beta]|1|[ndash]|induced epithelial-to-mesenchymal transition and reverses chronic renal injury. Nature medicine, 2003, 9(7): 964-968.
56.LEONARD EC, FRIEDRICH JL, BASILE DP. VEGF-121 preserves renal microvessel structure and ameliorates secondary renal disease following acute kidney injury. American Journal of Physiology-Renal Physiology, 2008, 295(6): F1648.
57.ZHANG SL, GUO J, MOINI B, et al. Angiotensin II stimulates Pax-2 in rat kidney proximal tubular cells:Impact on proliferation and apoptosis. Kidney International, 2004, 66(6): 2181.
58.STANISLAS F, NICOLAS M, AUDREY C, et al. Hnf-1β Transcription Factor Is an Early Hif-1α-Independent Marker of Epithelial Hypoxia and Controls Renal Repair. Plos One, 2013, 8(5): e63585.
59.BRAUN N, HAAP M, OVERKAMP D, et al. Characterization and outcome following Puumala virus infection:a retrospective analysis of 75 cases. Nephrol Dial Transplant, 2010, 25(9): 2997-3003.
60.SNAEDAL S, HEIMBüRGER O, QURESHI AR, et al. Comorbidity and acute clinical events as determinants of C-reactive protein variation in hemodialysis patients: implications for patient survival. American Journal of Kidney Diseases, 2009, 53(6): 1024-1033.
61.GAO F, ZHOU YJ, ZHU X, et al. C-reactive protein and the risk of contrast-induced acute kidney injury in patients undergoing percutaneous coronary intervention. American Journal of Nephrology, 2011, 34(3): 203.
62.TANG Y, HUANG XR, LV J, et al. C-reactive protein promotes acute kidney injury by impairing G1/S-dependent tubular epithelium cell regeneration. Clinical Science, 2014, 126(9): 645-659.
63.AWAD AS, ROUSE M, HUANG L, et al. Compartmentalization of neutrophils in the kidney and lung following acute ischemic kidney injury. Kidney International, 2009, 75(7): 689.
64.WANG Y, WANG YP, ZHENG G, et al. Ex vivo, programmed macrophages ameliorate experimental chronic in flammatory renal disease. Kidney International, 2007, 72(3): 290.
65.LEE S, HUEN S, NISHIO H, et al. Distinct Macrophage Phenotypes Contribute to Kidney Injury and Repair.Journal of the American Society of Nephrology Jasn, 2011, 22(2): 317-326.
66.JOHN R, NELSON PJ. Dendritic cells in the kidney. Journal of the American Society of Nephrology : JASN,2007, 18(10): 2628-2635.
67.ASCON DB, LOPEZ-BRIONES S, LIU M, et al. Phenotypic and functional characterization of kidneyin filtrating lymphocytes in renal ischemia reperfusion injury. Journal of Immunology, 2006, 177(5): 3380.
68.NOIRI E, DOI K, INAGI R, et al. Contribution of T lymphocytes to rat renal ischemia/reperfusion injury.Clinical & Experimental Nephrology, 2009, 13(1): 25-32.
69.HUEN SC, CANTLEY LG. Macrophage-mediated injury and repair after ischemic kidney injury. Pediatric Nephrology, 2015, 30(2): 199-209.
70.WILSON HM, WALBAUM D, REES AJ. Macrophages and the kidney. Current Opinion in Nephrology &Hypertension, 2004, 13(3): 285.
71.HAMID RABB, FRANK DANIELS, MICHAEL O’DONNELL, et al. Pathophysiological role of T lymphocytes in renal ischemia-reperfusion injury in mice. American Journal of Physiology-Renal Physiology,2000, 279(3): F525-F525.
72.CALDWELL CC, OKAYA T, MARTIGNONI A, et al. Divergent functions of CD4+ T lymphocytes in acute liver in flammation and injury after ischemia-reperfusion. American Journal of Physiology Gastrointestinal &Liver Physiology, 2005, 289(5): G969.
73.GANDOLFO MT, JANG HR, BAGNASCO SM, et al. Foxp3+ regulatory T cells participate in repair of ischemic acute kidney injury. Kidney International, 2009, 76(7): 717.
74.MOGHADASALI R, AZARNIA M, HAJINASROLLAH M, et al. Intra-renal arterial injection of autologous bone marrow mesenchymal stromal cells ameliorates cisplatin-induced acute kidney injury in a rhesus Macaque mulatta, monkey model. Cytotherapy, 2014, 16(6): 734-749.
75.SUSNIK N, S?RENSENZENDER I, RONG S, et al. Ablation of proximal tubular suppressor of cytokine signaling 3 enhances tubular cell cycling and modifies macrophage phenotype during acute kidney injury.Kidney International, 2014, 85(6): 1357-1368.
76.MAESHIMA A, ZHANG YQ, NOJIMA Y, et al. Involvement of the activin-follistatin system in tubular regeneration after renal ischemia in rats. Journal of the American Society of Nephrology Jasn, 2001, 12(8):1685.
77.MAESHIMA A, NOJIMA Y, KOJIMA I. Activin A: An autocrine regulator of cell growth and differentiation in renal proximal tubular cells. Kidney International, 2002, 62(2): 446-454.
78.GOBé G, ZHANG XJ, CUTTLE L, et al. Bcl-2 genes and growth factors in the pathology of ischaemic acute renal failure. Immunology and cell biology, 1999, 77(3): 279-286.
79.HE W, DAI C, LI Y, et al. Wnt/β-Catenin Signaling Promotes Renal Interstitial Fibrosis. Journal of the American Society of Nephrology Jasn, 2009, 20(4): 765.
80.HE W, KANG YS, DAI C, et al. Blockade of Wnt/β-catenin signaling by paricalcitol ameliorates proteinuria and kidney injury. Journal of the American Society of Nephrology Jasn, 2011, 22(1): 90.
81.LIN SL, LI B, RAO S, et al. Macrophage Wnt7b is critical for kidney repair and regeneration. Proc Natl Acad Sci USA, 2010, 107(9): 4194-4199.
82.HERRERA M, MIROTSOU M. Stem cells: potential and challenges for kidney repair. American journal of physiology. Renal physiology, 2014, 306(1): 12-23.
83.AGGARWAL S, MOGGIO A, BUSSOLATI B. Concise review: stem/progenitor cells for renal tissue repair:current knowledge and perspectives. Stem Cells Translational Medicine, 2013, 2(12): 1011.
84.SALLUSTIO F, COSTANTINO V, COX SN, et al. Human renal stem/progenitor cells repair tubular epithelial cell injury through TLR2-driven inhibin-A and microvesicle-shuttled decorin. Kidney International, 2013,83(3): 392.
85.JIN M, XIE Y, LI Q, et al. Stem cell-based cell therapy for glomerulonephritis. BioMed research international,2014, 2014(1): 124730.
86.MORIGI M, IMBERTI BC, CORNA D, et al. Mesenchymal stem cells are renotropic, helping to repair the kidney and improve function in acute renal failure. Journal of the American Society of Nephrology Jasn, 2004,15(7): 1794.
87.HAUSER PV, DE FR, BRUNO S, et al. Stem cells derived from human amniotic fluid contribute to acute kidney injury recovery. American Journal of Pathology, 2010, 177(4): 2011-2021.
88.ROTA C, IMBERTI B, POZZOBON M, et al. Human amniotic fluid stem cell preconditioning improves their regenerative potential. Stem Cells & Development, 2012, 21(11): 1911-1923.
89.WANG PR. Mouse adult renal progenitor cells in combination with erythropoietin or suramin-a potential new strategy for the treatment of acute kidney injury. Stem Cell Research & Therapy, 2013, 4(4): 1-2.
90.GRANGE C, MOGGIO A, TAPPARO M, et al. Protective effect and localization by optical imaging of human renal CD133+ progenitor cells in an acute kidney injury model. Physiological Reports, 2014, 2(5): e12009.
91.SMITH PL, BUFFINGTON DA, HUMES HD. Kidney epithelial cells. Methods Enzymol, 2006, 419(419):194-207.
92.STIENNONHEUSON JA.[Control of renal tubular regeneration]Bulletin Et Mémoires De Lacadémie Royale De Médecine De Belgique, 1992, 147: 89.
93.ZHU XY, URBIETA-CACERES V, KRIER JD, et al. Mesenchymal Stem Cells and Endothelial Progenitor Cells Decrease Renal Injury in Experimental Swine Renal Artery Stenosis Through Different Mechanisms.Stem Cells, 2013, 31(1): 117-125.
94.ROMAGNANI P. Kidney regeneration: any prospects? Contributions to nephrology, 2011, 170: 228.
95.KAYS SE, SCHNELLMANN RG. Regeneration of renal proximal tubule cells in primary culture following toxicant injury: response to growth factors. Toxicology & Applied Pharmacology, 1995, 132(2): 273.
96.DORRONSORO A, ROBBINS PD. Regenerating the injured kidney with human umbilical cord mesenchymal stem cell-derived exosomes. Stem Cell Research & Therapy, 2013, 4(2): 39.
97.CHHABRA P, BRAYMAN KL. The use of stem cells in kidney disease. Current opinion in organ transplantation, 2009, 14(1): 72.
98.XINARIS C, MORIGI M, BENEDETTI V, et al. A novel strategy to enhance mesenchymal stem cell migration capacity and promote tissue repair in an injury specific fashion. Cell Transplantation, 2013, 22(3): 423-436.
99.LIU N, TIAN J, CHENG J, et al. Migration of CXCR4 gene‐modified bone marrow‐derived mesenchymal stem cells to the acute injured kidney. Journal of Cellular Biochemistry, 2013, 114(12): 2677.
100.LIU N, TIAN J, CHENG J, et al. Effect of erythropoietin on the migration of bone marrow-derived mesenchymal stem cells to the acute kidney injury microenvironment. Experimental Cell Research, 2013,319(13): 2019-2027.
101.SAGRINATI C, RONCONI E, LAZZERI E, et al. Stem-cell approaches for kidney repair: choosing the right cells. Trends in Molecular Medicine, 2008, 14(7): 277-285.
102.BENJAMIN D. HUMPHREY S. Kidney Injury, Stem Cells and Regeneration. Current opinion in nephrology and hypertension, 2014, 23(1): 25-31.